Community events marking International Overdose Awareness Day on Aug. 31 come amid a series of local deaths which have slowed this year over last.
Advertisement 2
This advertisement has not loaded yet, but your article continues below.
Article content
Statistics show 28 people died by fentanyl or another opioid overdose in Grey-Bruce last year. But those are just coroner-confirmed cases.
There were actually 46 suspected drug deaths in Grey-Bruce last year but the cause has not been confirmed in all cases. So far this year there have been 20 suspected drug deaths, Grey Bruce Health Unit figures show.
Comparing May, June and July, there were eight suspected drug deaths last year and four this year.
So the pace of suspected drug deaths has slowed this year, said Alexis Cook, the health unit’s harm reduction manager responsible for responding to the opioid problem.
There was another suspected fatal opioid overdose in Owen Sound Thursday. The health unit has issued three overdose alerts this month, triggered when there are three or more overdoses in a 48-hour period.
Advertisement 3
This advertisement has not loaded yet, but your article continues below.
Article content
The person who died was in his or her mid-30s and Cook noted people aged 25 to 44 are three times more likely than any other age group to experience a fatal drug overdose. Local and provincial data both show that, she said.
Fatal drug overdoses peaked in 2020 during the pandemic, when more than 2,400 people in Ontario died. That was a 58 per cent increase over 2019, when 1,529 people died.
Cook said local figures indicate we all need to be aware of the ongoing drug overdose crisis. People can help by being trained and carrying naloxone kits containing the drug which temporarily reverses an opioid drug overdose.
Also, people should know the Good Samaritan Act protects people from simple drug possession charges when 911 is called, she said.
Advertisement 4
This advertisement has not loaded yet, but your article continues below.
Article content
Cook said the health unit is “currently working with community partners to build a response, as it is a priority for public health, and to increase our current response.” Public health nurses visited drug users in the community during each of the three overdose alerts this month, Cook said.
“The nurses went out and they did targeted outreach and ensured that individuals who were using drugs had access to naloxone . . . we hand out needles as well and we do meth kits and crack kits to ensure individuals are using as safely as possible.”
The nurses reminded them to use drugs with someone else present who can administer naloxone, or use while on the line with an operator with the Overdose Prevention Line, who will call 911 if the user becomes unresponsive, she said.
Advertisement 5
This advertisement has not loaded yet, but your article continues below.
Article content
Naloxone is available free-of-charge at the health unit Monday to Friday and from community partners, including paramedics and mental health workers.
To mark International Overdose Awareness Day, there will be a community barbecue at Neyaashiinigmiing on Tuesday, the day before the official day for overdose awareness, from 2 p.m. until sunset, at Kina Waa Noojmojig Nanaweing Wellness Pavilion.
Owen Sound will have three events: a community barbecue from noon to 3 p.m. at Safe ‘n Sound drop-in centre, a barbecue and sacred fire from 3 p.m. to 5 p.m. at M’Wikwedong Indigenous Friendship Centre, and a candlelit vigil from 6:30 p.m. to 8:30 p.m. at the Owen Sound Farmers’ Market parking lot.
Also Aug. 31, a candlelit vigil will take in Port Elgin at Coulter Parkette, and a candlelit vigil with speakers will take place in Hanover’s Hope Community Church from 6:30 p.m. to 8:30 p.m., to which people are asked to bring a blanket or lawn chair.
“These events are a chance to stimulate discussion about substance use prevention, overdose prevention, available supports and evidence-based drug policies and reduce the stigma of drug-related deaths,” Cook said in a news release. “It’s also a time for the community to mourn, in a safe environment, and remember the loved ones who have been lost.”
Myocardial infarction mortality varies substantially within high-income countries. There is limited guidance on what interventions—including primary and secondary prevention, or improvement of care pathways and quality—can reduce myocardial infarction mortality. Our aim was to understand the contributions of incidence (event rate), pre-hospital deaths, and hospital case fatality to the variations in myocardial infarction mortality within England.
Methods
We used linked data from national databases on hospitalisations and deaths with acute myocardial infarction (ICD-10 codes I21 and I22) as a primary hospital diagnosis or underlying cause of death, from Jan 1, 2015, to Dec 31, 2018. We used geographical identifiers to estimate myocardial infarction event rate (number of events per 100 000 population), death rate (number of deaths per 100 000 population), total case fatality (proportion of events that resulted in death), pre-hospital fatality (proportion of events that resulted in pre-hospital death), and hospital case fatality (proportion of admissions due to myocardial infarction that resulted in death within 28 days of admission) for men and women aged 45 years and older across 326 districts in England. Data were analysed in a Bayesian spatial model that accounted for similarities and differences in spatial patterns of fatal and non-fatal myocardial infarction. Age-standardised rates were calculated by weighting age-specific rates by the corresponding national share of the appropriate denominator for each measure.
Findings
From 2015 to 2018, national age-standardised death rates were 63 per 100 000 population in women and 126 per 100 000 in men, and event rates were 233 per 100 000 in women and 512 per 100 000 in men. After age-standardisation, 15·0% of events in women and 16·9% in men resulted in death before hospitalisation, and hospital case fatality was 10·8% in women and 10·6% in men. Across districts, the 99th-to-1st percentile ratio of age-standardised myocardial infarction death rates was 2·63 (95% credible interval 2·45–2·83) in women and 2·56 (2·37–2·76) in men, with death rates highest in parts of northern England. The main contributor to this variation was myocardial infarction event rate, with a 99th-to-1st percentile ratio of 2·55 (2·39–2·72) in women and 2·17 (2·08–2·27) in men across districts. Pre-hospital fatality was greater than hospital case fatality in every district. Pre-hospital fatality had a 99th-to-1st percentile ratio of 1·60 (1·50–1·70) in women and 1·75 (1·66–1·86) in men across districts, and made a greater contribution to variation in total case fatality than did hospital case fatality (99th-to-1st percentile ratio 1·39 [1·29–1·49] and 1·49 [1·39–1·60]). The contribution of case fatality to variation in deaths across districts was largest in women aged 55–64 and 65–74 years and in men aged 55–64, 65–74, and 75–84 years. Pre-hospital fatality was slightly higher in men than in women in most districts and age groups, whereas hospital case fatality was higher in women in virtually all districts at ages up to and including 65–74 years.
Interpretation
Most of the variation in myocardial infarction mortality in England is due to variation in myocardial infarction event rate, with a smaller role for case fatality. Most variation in case fatality occurs before rather than after hospital admission. Reducing subnational variations in myocardial infarction mortality requires interventions that reduce event rate and pre-hospital deaths.
Funding
Wellcome Trust, British Heart Foundation, Medical Research Council (UK Research and Innovation), and National Institute for Health Research (UK).
Introduction
Mortality from ischaemic heart disease has declined substantially in high-income countries, driven by both a decline in incidence and improved survival of myocardial infarction—the acute presentation of ischaemic heart disease which has the potential to be rapidly fatal in the absence of appropriate interventions.
Determinants of the decline in mortality from acute myocardial infarction in England between 2002 and 2010: linked national database study.
This decrease in incidence of myocardial infarction has been due to reductions in risk factors such as smoking, blood pressure, and cholesterol in the population, as well as primary and secondary prevention through pharmacological treatment in individuals at high risk.
Contributions of risk factors and medical care to cardiovascular mortality trends.
Improvement in myocardial infarction survival has been achieved by more rapid diagnosis and revascularisation and through the use of anti-platelet agents based on evidence from randomised trials. At the health-system level, the establishment of cardiology wards, coronary care units, and cardiac intensive care units, staffed by specialist cardiac doctors and nurses, has helped to standardise and optimise the delivery of the aforementioned treatments and to identify and intervene on complications early.
A tale of coronary artery disease and myocardial infarction.
Research in context
Evidence before this study
We searched MEDLINE (via PubMed) for articles published from Jan 1, 2000, to Dec 6, 2021, using the search terms (“myocardial infarction”[Title] OR “coronary heart disease”[Title] or “ischaemic heart disease”[Title]) AND ((“subnational”) OR (“small area”) OR (“local”)) AND ((“registry”) OR (“incidence”) OR (“mortality”) OR (“case fatality”)). No language restrictions were applied. We started our search from the year 2000 in order to focus on studies after the introduction of primary angioplasty and the use of troponin-based measurements to define myocardial infarction. We also searched for relevant reports through the websites of registries and requests for information from clinicians and researchers in high-income countries in Australasia, Europe, and the Americas. We found some studies from countries in Australasia, Europe, and the Americas that had used data on hospitalised patients and reported myocardial infarction admissions and hospital case fatality for an entire country. The Organisation for Economic Co-operation and Development also reports hospital case fatality for its member states based on countries’ officially reported statistics, but the actual data sources are not stated. Few of these studies included deaths outside of a hospital setting; of these, some had considered all ischaemic heart disease deaths, and only four national studies had specifically focused on pre-hospital acute myocardial infarction deaths. We also found a study that used data from specific communities in six countries to report on myocardial infarction admissions and pre-hospital and hospital case fatality, as had been done in the MONICA study for the 1990s. In terms of subnational studies, we found one study on death rates for ischaemic heart disease for US counties, and two reports of ischaemic heart disease death rates for local authorities in England. These studies did not separate pre-hospital versus hospital fatality or distinguish acute myocardial infarction from chronic atherosclerotic disease and complications; nor did they have data on hospitalisation. We also found one local authority-level study of myocardial infarction hospitalisation rates in England, but this study did not include pre-hospital deaths. To our knowledge, there is no study on subnational variations in myocardial infarction death rate and its complete contributors (event rates, pre-hospital fatality, and hospital case fatality).
Added value of this study
To our knowledge, this study provides the only subnational analysis of myocardial infarction death rate and its complete contributors in any country. We used nationwide linked data that capture all forms of myocardial infarction events: non-fatal events and pre-hospital and hospital fatality. We used a spatial statistical model to obtain stable estimates of myocardial infarction event rates and pre-hospital fatality and hospital case fatality by age group for small geographies, together with the uncertainty in these estimates.
Implications of all the available evidence
Our subnational results, together with available national data, show that pre-hospital deaths are a larger contributor to myocardial infarction mortality, and how it varies both within and across high-income countries, than is hospital case fatality. This finding demonstrates the need for research on, and implementation and standardisation of, interventions that reduce time between symptom onset and call for help, as well as the time to initiation of cardiopulmonary resuscitation and defibrillation in the event of a myocardial infarction leading to cardiac arrest. There is also a need for regular national and subnational reporting of all myocardial infarction deaths, separated by whether the individual had a recent hospital admission, so that the impacts of interventions can be measured.
Despite these aggregate successes, ischaemic heart disease mortality varies markedly within high-income countries, including in England, and the available data indicate that mortality due to myocardial infarction is a major contributor to this variation.
Chapter 12: geographic variation in mortality by social class and alternative social classifications.
Myocardial infarction mortality, and its variation within a population, can be reduced through primary and secondary prevention measures to reduce event rates; improving awareness of myocardial infarction symptoms and initial response time to reduce the share of patients with myocardial infarction who die before reaching a hospital; and improving hospital care. Many current trial and standardisation efforts are targeted towards the latter component.
A tale of coronary artery disease and myocardial infarction.
However, there are limited data on the relative importance of these three contributors to subnational variations in myocardial infarction mortality, which are needed to inform the selection of optimal strategies for reducing myocardial infarction mortality where it is high.
We used linked data on hospitalisations and deaths in England’s 326 local authority districts (political and administrative units that are used for the allocation of public health and social care budgets and for the formulation and delivery of primary prevention; referred to henceforth as districts) to determine how much the geographical variation in myocardial infarction mortality arises from variations in event rates and in case fatality and its constituents, namely pre-hospital death and death following hospitalisation (referred to as hospital case fatality).
Results
From 2015 to 2018, there were 293 715 myocardial infarction hospitalisations and 87 966 myocardial infarction-related deaths in England among people aged 45 years or older. Of these deaths, 76 011 (86·4%) had acute myocardial infarction as the underlying cause of death and the remaining 11 955 (13·6%) were deaths assigned to other causes within 28 days of a myocardial infarction admission (appendix pp 6–9). Of the 76 011 deaths with myocardial infarction as the underlying cause, 19 294 (25·4%) occurred within 28 days of a myocardial infarction admission, 20 510 (27·0%) occurred within 28 days of a non-myocardial infarction admission, and 36 207 (47·6%) had no preceding admission. 262 466 (89.3%) of the total myocardial infarction hospitalisations were non-fatal. The national age-standardised myocardial infarction death rate (calculated directly from death and population counts) was 63 per 100 000 population in women and 126 per 100 000 in men, and the national age-standardised event rate was 233 per 100 000 in women and 512 per 100 000 in men. Pre-hospital fatality was 15·0% in women and 16·9% in men, and hospital case fatality was 10·8% in women and 10·6% in men.
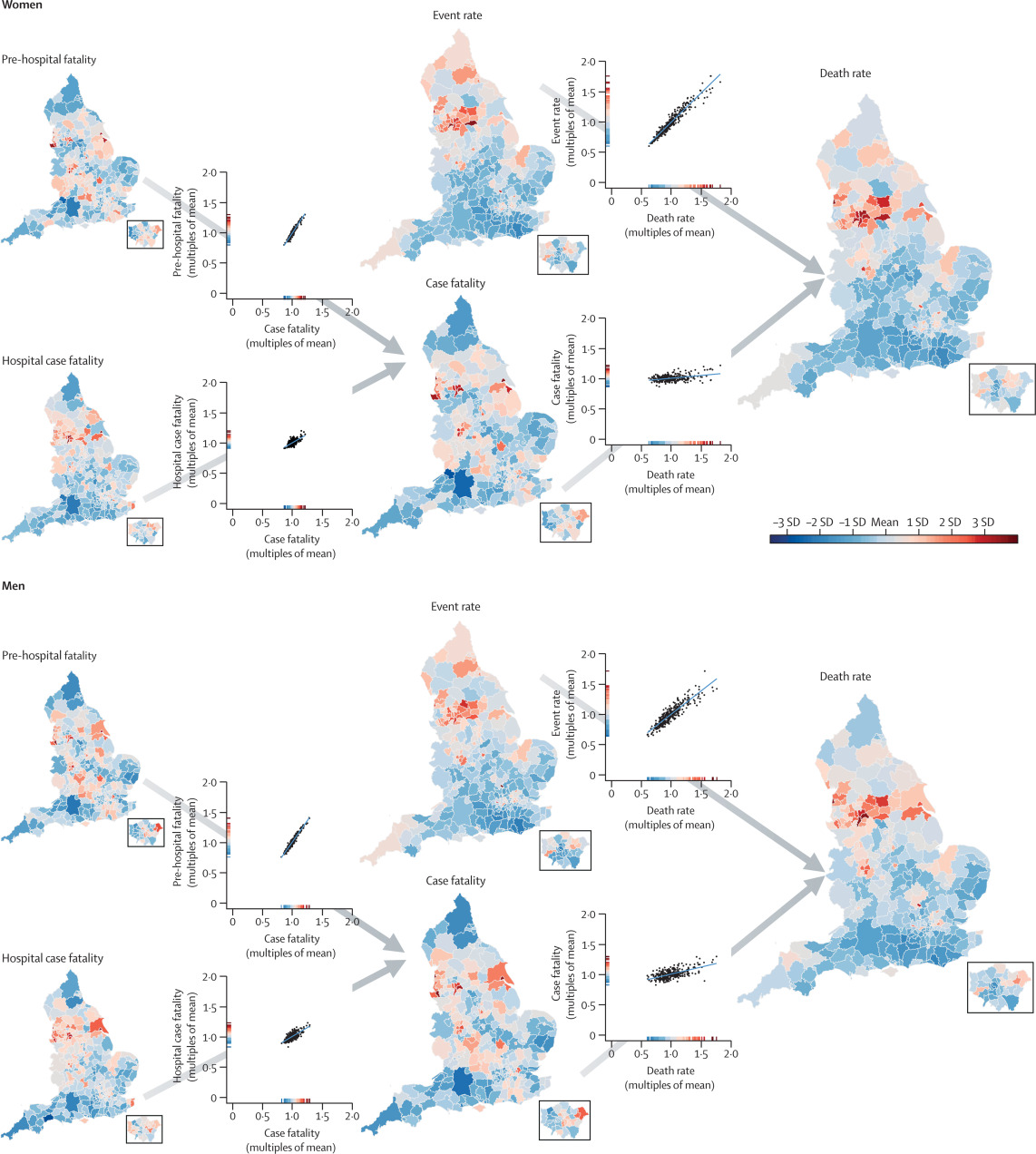
The geographical patterns and variations of myocardial infarction mortality and its contributors are shown in figure 1 and in the appendix (pp 10–13). Of contributors to mortality, event rate varied the most, with 99th-to-1st percentile ratios of 2·55 (95% CrI 2·39–2·72) in women and 2·17 (2·08–2·27) in men, compared with 1·36 (1·31–1·43) in women and 1·50 (1·44–1·57) in men for case fatality (table 1). Myocardial infarction mortality was strongly correlated with event rates (correlation coefficients 0·96 for women and 0·91 for men), but only moderately correlated with case fatality (0·39 and 0·61), making event rate the largest driver of the variation in myocardial infarction mortality (99th-to-1st percentile ratio 2·63 [2·45–2·83] in women and 2·56 [2·37–2·76] in men).
Figure 1Age-standardised acute myocardial infarction death rate and its contributors in districts of England in women and men
The maps show the geography of death rate and each contributor (insets show London). The scatter plots show the relationship between pairs of contributors, or contributors and death rates. All variables were age-standardised. The scale on each scatter plot ranges from 0 to 2 × the mean of the values across all districts to allow the extent of variation to be compared among variables. The colour corresponds to the number of SDs above or below the mean value across all districts. The appendix shows maps and scatter plots with numerical scales (pp 10–11) and the posterior probabilities that the estimated rates and case fatality for each district are higher or lower than the national average (pp 12–13).
Table 1Distributions of myocardial infarction mortality and its components (event rate and case fatality, including pre-hospital fatality and hospital case fatality) across 326 districts in England
Mortality, event rate, and fatality all apply to myocardial infarction. Numbers in parentheses are 95% credible intervals. The best performing and worst performing districts (ie, the individual districts with the lowest and highest values, respectively) could be different for each outcome.
Variation in total case fatality across districts was driven more by the variation in pre-hospital fatality (99th-to-1st percentile ratio 1·60 [1·50–1·70] in women and 1·75 [1·66–1·86] in men) than hospital case fatality (1·39 [1·29–1·49] and 1·49 [1·39–1·60]). In all 326 districts, pre-hospital fatality was higher than hospital case fatality, by an average factor of 1·40 in women and 1·59 in men (figure 2). Mortality was highest in a cluster of urban districts in the north of England. These districts stood out as having distinctly high myocardial infarction event rates compared with most other districts in England, but were less consistently high with regard to case fatality. For example, Barnsley, Salford, and Luton had higher-than-average event rates in women but lower-than-average case fatality (average refers to the mean across districts for each outcome). Similarly, places such as Luton, Blackburn, Middlesbrough, Hounslow, and County Durham had higher-than-average event rates in men, driving their high death rates, whereas their case fatality was lower than average (figure 1).
Figure 2Relationship between pre-hospital fatality and hospital case fatality
Myocardial infarction mortality increased by more than 3-fold per decade of age for women and more than 2-fold for men (figure 3). This increase was a result of a rise in both event rates (2·10-fold higher per decade of age for women and 1·61-fold for men) and case fatality, which increased by around 50% per decade of age. The age association of case fatality was more similar to that of pre-hospital fatality (an increase per decade of 1·40-fold in women and 1·38-fold in men) than hospital case fatality (1·75-fold in women and 1·87-fold in men), because the number of pre-hospital deaths exceeded that of deaths following hospitalisation in every age group.
Figure 3Distribution of myocardial infarction mortality, event rates, pre-hospital fatality, and hospital case fatality by age group and sex, and male-to-female ratios
Each point represents one district. *Percentage of all myocardial infarction events. †Percentage of all myocardial infarction hospital admissions.
Myocardial infarction death rate was higher in men than in women in every age group and for all districts. Event rate was also consistently higher in men than in women, in all except two districts in the oldest age groups (75–84 and ≥85 years). In some districts, death and event rates in men exceeded those in women by more than five times in the 45–54 and 55–64 years age groups, and up to four times in those aged 65–74 years. Pre-hospital fatality was slightly higher in men than in women in most districts and age groups, whereas hospital case fatality was higher in women in almost all districts in the 45–54 years and 55–64 years age groups; in higher age groups, it was more similar between the sexes (figure 3).
In all age groups, variation in event rates made a greater contribution to how much myocardial infarction mortality varied across districts than did variation in case fatality (table 2). The relative importance of case fatality was highest in women aged 55–64 and 65–74 years and in men aged 55–64, 65–74, and 75–84 years, and was lowest in the youngest age groups (in which case fatality is low in all districts) and the oldest age groups (in which case fatality is high in all districts).
Table 2Proportion of variation in myocardial infarction mortality across districts explained by myocardial infarction event rates and case fatality, by sex and age group
Percentages show how much less variable myocardial infarction death rates would be if that contributor (event rate or case fatality) was at the same level in all districts in that age-sex group. Myocardial infarction event rates and case fatality act in a multiplicative manner in each district to produce the death rate and are not independent; thus, the contributions do not add to 100%.
Myocardial infarction death rate and event rate were directly associated with district-level income deprivation (figure 4). For pre-hospital fatality and hospital case fatality, the distributions were similar for most deciles, except for the poorest 20% of districts. In these two deciles, higher proportions of myocardial infarction events led to death before reaching a hospital and higher proportions of hospitalised patients died than in the other districts. The variation in death rates, event rates, and fatality were all larger within each decile of income deprivation than across the deciles.
Figure 4Distribution of myocardial infarction mortality, event rates, pre-hospital fatality, and hospital case fatality by decile of income deprivation
Each point represents one district. *Percentage of all myocardial infarction events. †Percentage of all myocardial infarction hospital admissions.
Sensitivity analyses showed that inclusion of all acute myocardial infarction deaths within 28 days of any admission (regardless of whether the primary admission diagnosis was myocardial infarction or another condition; an additional 25 510 deaths) as post-hospitalisation deaths increased hospital case fatality by 4·7–8·2 percentage points and decreased pre-hospital fatality by 4·4–8·2 percentage points across different districts and the two sexes. As a result, the degree of variation in pre-hospital fatality among districts increased, but the overall ranking of districts in terms of high versus low hospital case fatality and pre-hospital fatality was maintained; the correlation coefficients between the results of the main and sensitivity analyses were 0·93 (women) and 0·95 (men) for district-level hospital case fatality, and 0·91 (women) and 0·94 (men) for district-level pre-hospital fatality.
All outcomes were correlated between the analyses done with and without including people aged 85 years and older. Correlation coefficients between the two age groups (≥45 years and 45–85 years) ranged from 0·96 to 0·99 for death rates and event rates in the two sexes, and from 0·89 to 0·96 for total case fatality, pre-hospital fatality, and hospital case fatality, possibly because case fatality is much higher in the oldest ages (figure 3).
Discussion
We found that variation in hospital case fatality made only a small contribution to the substantial geographical variation in myocardial infarction mortality in England from 2015 to 2018. A much bigger element of this variation in mortality arose from pre-hospital deaths and event rates. Hospital case fatality, nonetheless, varied across districts.
Our results are based on nationwide linked data that capture all forms of myocardial infarction: non-fatal, and pre-hospital and post-admission fatal. These distinctions are key to designing and evaluating interventions that target the most important determinants of mortality. The use of routine health-care data, while enabling a national analysis, has some limitations. ICD-10 codes summarise diagnoses but do not specify clinical investigations and laboratory results. Thus, ST-elevation myocardial infarction (STEMI) and non-STEMI cannot be definitively distinguished. The assignment of ICD-10 codes might also vary across physicians and hospitals. Nonetheless, the quality and consistency of coding of myocardial infarction in routine hospital data have been evaluated against clinical disease registries and chart reviews of myocardial infarction using established diagnostic criteria, with sensitivity and positive predictive values reported to be 79–95%, and hospitalisation data having higher validity than mortality statistics.
Validity of myocardial infarction diagnoses in administrative databases: a systematic review.
We did not include cases of myocardial infarction diagnosed as a secondary condition because the recording of secondary diagnoses is more variable than that of primary diagnoses, and the causes of secondary myocardial infarction, as well as the treatment pathways, might differ. Nationally, the inclusion of cases of myocardial infarction recorded as a secondary diagnosis would lead to around a 37% increase in total myocardial infarction admissions.
Acute myocardial infarction hospital admissions and deaths in England: a national follow-back and follow-forward record-linkage study.
Cause-of-death assignment is based on more limited clinical information than hospital diagnostic codes—eg, in cases of pre-hospital cardiac arrest—and thus might be more subject to error.
Validity of myocardial infarction diagnoses in administrative databases: a systematic review.
It is unlikely, however, that cause-of-death assignment varies subnationally enough to affect the results.
To our knowledge, no previous study has analysed small-area variation in myocardial infarction deaths and its constituents (non-fatal events and pre-hospital and post-admission deaths). Some studies have reported national data for specific countries; most of these studies relied on data from hospitalised patients (ie, excluding pre-hospital deaths),
Short-term and long-term outcomes in 133,429 emergency patients admitted with angina or myocardial infarction in Scotland, 1990–2000: population-based cohort study.
25 year trends in first time hospitalisation for acute myocardial infarction, subsequent short and long term mortality, and the prognostic impact of sex and comorbidity: a Danish nationwide cohort study.
A national record linkage to study acute myocardial infarction incidence and case fatality in Sweden.
there is little comparative data on total case fatality and especially on the percentage of events that lead to death before hospitalisation. Consistent with our finding across districts, these studies found that pre-hospital fatality was a larger contributor to case fatality than was hospital case fatality. Pre-hospital fatality also varied more across countries than did hospital case fatality.
The current standard of care for myocardial infarction in England and other nations is resuscitation, early diagnosis with electrocardiography, and rapid transfer of patients with STEMI to a percutaneous coronary intervention centre for immediate revascularisation. Reorganisation of emergency services to facilitate rapid transfer, reduction in door-to-balloon reperfusion times, and universal anti-platelet therapy are among the reasons for hospital case fatality having the least variation among the constituents of myocardial infarction mortality, both within England and across high-income countries. The remaining variations in hospital case fatality might be partly due to differences in reperfusion times and percutaneous coronary intervention capacity, adherence to guidelines, or patient comorbidities.
Evaluation of the impact of the GRACE risk score on the management and outcome of patients hospitalised with non-ST elevation acute coronary syndrome in the UK: protocol of the UKGRIS cluster-randomised registry-based trial.
National Institute for Clinical Outcomes Research Myocardial ischaemia national audit project (MINAP): 2020 summary report (2018/2019 data).
Management of non-STEMI, which relies on risk stratification to decide on early versus delayed angiography and on optimal anti-coagulant and anti-platelet therapy, also accounts for some of the observed variations in hospital case fatality.
Evaluation of the impact of the GRACE risk score on the management and outcome of patients hospitalised with non-ST elevation acute coronary syndrome in the UK: protocol of the UKGRIS cluster-randomised registry-based trial.
Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies SWEDEHEART annual report 2020.
Excess mortality and guideline-indicated care following non-ST-elevation myocardial infarction.
Finally, the use of secondary prevention therapies in the immediate post-myocardial infarction phase, which improves both 28-day and longer-term survival, also varies within England and across countries.
Excess mortality and guideline-indicated care following non-ST-elevation myocardial infarction.
As hospital case fatality has declined and become less variable, pre-hospital fatality plays a larger relative role in the survival of patients and its variations across and within countries. Important determinants of pre-hospital fatality include the time taken to recognise symptoms and call for and receive help, and the use of pre-hospital cardiopulmonary resuscitation (CPR) and pre-hospital defibrillation in the event of cardiac arrest.
Impact of a public awareness campaign on out-of-hospital cardiac arrest incidence and mortality rates.
but these programmes are rarely targeted and adapted to communities where pre-hospital deaths are high. Strategies to reduce mortality from cardiac arrest following myocardial infarction
European first responder systems and differences in return of spontaneous circulation and survival after out-of-hospital cardiac arrest: a study of registry cohorts.
increasing the number of public-access defibrillators;
The use of trained volunteers in the response to out-of-hospital cardiac arrest—the GoodSAM experience.
The available data show that some of the potentially effective interventions, such as public-access defibrillators, are used less commonly than standardised facility-level interventions; the use of other interventions, such as bystander CPR, varies across and within countries.
Survival after out-of-hospital cardiac arrest in Europe—results of the EuReCa TWO study.
Alongside lowering case fatality where it remains high, our results show that there is a need and potential to further reduce myocardial infarction event rates in many parts of England because the sheer size of case numbers can drive areas that benefit from low case fatality into high mortality rankings, and vice versa. Event rates are influenced by smoking and risk factors such as blood pressure, lipid levels, diabetes, and obesity, which mediate the effects of nutrition and the environment. In England, these risk factors tend to be higher where myocardial infarction event rates are highest.
Healthier central England or North-South divide? Analysis of national survey data on smoking and high-risk drinking.
These risks can be partly reduced through more ambitious and equitable preventive interventions, such as New Zealand’s recent zero-smoking policy and financial support for healthy foods.
Strengthening the public health impacts of the supplemental nutrition assistance program through policy.
Risk can also be effectively mitigated by individual-level primary and secondary prevention through counselling for smoking cessation, statin therapy, and treatment of hypertension and diabetes. In England, cardiovascular risk screening has been offered to approximately 33% of the eligible population, of whom only about 50% take it up, leaving many of those at risk unscreened and untreated; the extent of undertreatment varies across the country.
Evaluation of the uptake and delivery of the NHS Health Check programme in England, using primary care data from 9.5 million people: a cross-sectional study.
The NHS Health Check in England: an evaluation of the first 4 years.
The decline in myocardial infarction mortality over the past five decades, driven by lower levels of smoking and other risk factors and advances in treatment both in primary care and specialist hospitals, has been a major clinical and public health success in high-income nations. Hospital case fatality is the element of the acute myocardial infarction pathway that is most relevant to those myocardial infarction patients who reach a facility, and most amenable to direct health-system intervention. However, with standardisation of hospital care following randomised trials, hospital case fatality now makes a smaller contribution to variations in myocardial infarction mortality within England and across high-income nations than do pre-hospital deaths and event rates. Nonetheless, the combination of our results and data on cross-country variations in hospital fatality show that further improvement in England is possible but requires a subnational focus where hospital case fatality remains high.
Our results also show that further scaling up population-based and individual-level primary and secondary prevention, as well as addressing the relatively large and highly variable pre-hospital fatality, are essential to reducing overall mortality. Strategies to achieve these reductions should be evaluated in randomised trials and in real-world conditions when new programmes are implemented. To ensure that these interventions translate to beneficial impact on death rates, there should be focus on parts of the country where each constituent of mortality is highest, and enhancement of registries to gather data on deaths outside the hospital setting, as currently done for hospitalised patients.
PA, PE, and ME conceived and designed the study. PA, HID, MD, and DF obtained and managed the data. PA, JEB, and ME developed the analytical strategy. PA conducted analysis in consultation with JEB and TR. PA, ME, JEB, and DPF interpreted the data and drafted the figures. PA and ME wrote the first draft of the manuscript. Other authors provided input to finalise the paper. PA, JEB, TR, and HID had full access to all data used in this study. PA and HID checked and verified the data used in the analysis. Due to data permission restrictions, not all authors were able to access the underlying data used in the study. All authors were responsible for submitting the article for publication.
Acknowledgments
We thank Andrew Moran (Resolve to Save Lives), Annika Rosengren (University of Gothenburg), Anoop Shah (London School of Hygiene & Tropical Medicine), Darwin Labarthe (Northwestern University), Jean-Michel Gaspoz (Geneva University Medical School), Johan Sundstrom (Upsala University), Rod Jackson (University of Auckland), Tomasz Zdrojewski (Medical University of Gdansk), Yuan Lu (Yale University), and Ziad Obermeyer (University of California Berkley) for their suggestions for the Discussion section. We thank Vasilis Kontis (Imperial College London) for insights on the implementation of the statistical model. PA was supported by a Wellcome Trust Clinical PhD Fellowship (grant number 092853/Z/10/Z). TR was supported by an Imperial College President’s PhD scholarship. Funding was also provided by the British Heart Foundation (Centre of Research Excellence grant RE/18/4/34215), the Wellcome Trust (Pathways to Equitable Healthy Cities grant 209376/Z/17/Z), the Medical Research Council (MRC Centre for Environment and Health grant MR/S019669/1 and grant MR/V034057/1) and the National Institute for Health Research (NIHR) Imperial College Biomedical Research Centre. PE acknowledges support from the Dementia Research Institute at Imperial College. The study uses the UK Small Area Health Statistics Unit (SAHSU) data, obtained from NHS Digital and the ONS. SAHSU holds approval from the Health Research Authority Confidentiality Advisory Group under regulation 5 of the health service (Control of Patient Information) regulations 2002 (section 251; reference 20/CAG/0028), and the National Research Ethics Service: London-South East Research Ethics Committee (reference 22/LO/0256). The work of SAHSU is funded by the UK Medical Research Council, Public Health England (now UK Health Security Agency), and the NIHR through Health Protection Units at Imperial College London in Environmental Exposures and Health (NIHR-200880) and in Chemical and Radiation Threats and Hazards (NIHR-200922). This Article does not necessarily reflect the views of Public Health England or the Department of Health.
Even as the National Centre for Disease Control (NCDC) has developed a surveillance system to record each death during extreme heat events, it also needs to be integrated in the public health system, experts have said.
Prof Mahaveer Golechha, Nodal officer of Centre for Excellence on Heat Health under the National Programme on Climate Change and Public Health, Union Ministry of Health and Family Welfare, Government of India, told The Indian Express that surveillance systems have been developed to record deaths during extreme heat events but are yet to be integrated in the public health system.
Prof Dileep Mavalankar, who heads the Indian Institute of Public Health at Gandhinagar, has said that hospital admissions and mortality need to be reported every day so that they can be correlated with heat. “What we have shown in Ahmedabad is that if you correlate mortality with temperature, then one can arrive at a local threshold. Each city has to have a local threshold of morbidity and mortality determination. Training and awareness programmes are being conducted but there is a need to record the death and correlate it with temperature across each city,” he said.
A National Action Plan on Heat-Related Illness (HRI) has been developed that outlines the basics of heat wave, HRIs and their management from primary to tertiary level, preparedness plan before, during and after summer season, and the standard operating procedures for surveillance of heat stroke cases and deaths. The plan has been prepared under the National Programme on Climate Change and Human Health. According to Dr Archana Patil, Maharashtra director of health, advisories along with weekly IMD weather bulletins on heat wave conditions have been issued to each district in the state as hot days become the norm across Maharashtra. “So far, no case of heat stroke has been reported this year,” state health authorities have said.
Dr Pradeep Awate, State surveillance officer, told The Indian Express that since the beginning of March there has been a rise in the maximum and minimum temperatures. Each district has been told to step up measures to come out with their heat action plans so that facilities like cooling rooms, emergency medical kits and others are in place. “With the help of IMD, we are also planning to step up awareness about the heat condition during a particular day with colour-based codes. White colours would be associated with normal, pleasant temperature. Yellow, orange and red colours would be associated with related alerts on mild and severe heat conditions,” Dr Awate added.
Dr Sanjay Deshmukh, Assistant Director (health) Pune circle, which includes Pune, Satara and Solapur, said weather bulletins were being shared with health authorities so that they were aware of the heat wave warning for the next five days.
New figures published today from the National Records of Scotland show birth rates continuing to decrease, death rates increasing, and the number of marriages rising beyond pre-pandemic levels.
Key findings from the latest quarterly report show:
There were 12,284 births registered in Scotland between 1 October and 31 December 2021. This is 3.6 per cent lower than the quarter four average of 12,742 over the five years 2015-2019.
At 17,297, the number of deaths in 2021 quarter four is 17.1 per cent higher than the quarter four average of 14,777 for 2015-2019.
The age-standardised mortality rate for the four-quarter period ending in 2021 quarter 4 was 0.6 per cent higher than the previous four-quarter period (ending 2021 quarter 3). This rate takes into account the growing and ageing population and is therefore the best indicator of the direction of the mortality trend.
There were 6,793 marriages. This was 12% higher than the average number of fourth quarter marriages over the five years 2015-2019.
There were 254 same-sex marriages, compared with a five-year average of 238.
Since June 2021 mixed-sex couples have been able to form a civil partnership. Of the 193 civil partnerships registered in the fourth quarter of 2021, 173 involved mixed-sex couples.
There were 20 same-sex civil partnerships, the same as the average 2015-2019.
Julie Ramsay, Vital Events statistician, said:
“Whilst the birth rate continued to fall and deaths were higher than the pre-pandemic average for the time of year, the number of marriages increased.
“12% more people got married in Scotland between October and December than the five year average for that time of year, coinciding with pandemic restrictions easing.”
There were 254 same-sex marriages, an increase on the five year average of 238, and of the 193 civil partnerships registered, 173 involved mixed-sex couples. The number of same-sex civil partnerships remained in line with the five year average”
The full publication ‘Births, deaths and other vital events, fourth quarter 2021’ is available on the NRS website. The report provides figures for vital events which were registered in Scotland in the period 1 October – 31 December 2021. The data includes statistics on births, stillbirths, marriages, civil partnerships and deaths, including:
Quarterly figures for Scotland for each of the past 10 years
The totals for each Local Authority and NHS Board area for the latest quarter
More details analyses of the numbers of deaths for the latest quarter
Figures are provisional and might be subject to further revision. Figures for 2021 will be finalised when the annual vital events reference tables are published in summer 2022.
Comparisons are usually made by comparing the current year to the average of the previous five years. For 2021, standard practice would be to compare against the 2016-2020 average. However, as the 2020 figures were severely affected by the COVID-19 pandemic – marriages were much lower than usual, deaths were higher, and registration of births was delayed – comparing 2021 figure to the 2016-2020 average would not give a true reflection of how the latest quarter’s figures compare to the average. Comparisons have therefore been made against the 2015-2019 average.
National Records of Scotland (NRS) is a non-ministerial department of the Scottish Government. It is responsible for producing statistics on Scotland’s population. General information about NRS’s statistics can be found in the About our Statistics section of its website.
Media enquiries should be directed to: Donna Green – 07775 027 380 NRS Communications Email: [email protected]
Further information about the statistics is available from: NRS Customer Services Email: [email protected]